
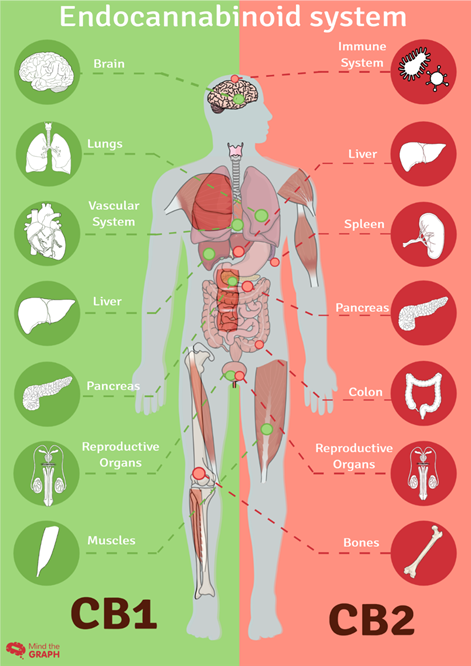
Picture Shows The Endocannabinoid Systems’ CB1 and CB2 Receptors; Which Are Both Stimulated By CBD and THC Cannabis
By Smoking Chef
What We Now Know
The endocannabinoid system (ECS) was discovered relatively recently, in the late 20th century. The key milestones in its discovery are as follows:
- 1964: The first major step was the isolation of Delta-9-tetrahydrocannabinol (THC), the main psychoactive compound in cannabis, by Dr. Raphael Mechoulam and his Colleagues. This groundbreaking work laid the foundation for further understanding the effects of cannabis on the body.
- 1988: The first cannabinoid receptor, CB1, was discovered by Allyn Howlett and William Devane. They identified these receptors in the brains of rats, and later it was found that they are also present in humans.
- 1992: The second cannabinoid receptor, CB2, was discovered by Dr. Raphael Mechoulam and colleagues. This receptor was primarily found in the immune system and peripheral tissues.
- 1995: The first endogenous cannabinoid compound, anandamide, was discovered by Dr. Raphael Mechoulam and his team. Anandamide was the first indication that the body produces its own compounds that interacts with the same receptors as THC.
- 1997: Another endogenous cannabinoid compound, 2-arachidonoylglycerol (2-AG), was discovered by researchers, Simon Ben-Shabat, Lumir Hanus, and colleagues. This further solidified the understanding of the endocannabinoid system and its role in the body. These discoveries collectively led to the establishment of the endocannabinoid system as a complex signaling system in the body that plays a role in regulating various physiological processes, including pain sensation, mood, appetite, immune function, and more. The understanding of the ECS has since continued to evolve, and research in this field is ongoing.
American Cannabis History Of The 19th And 20th Century
Between 1842 and 1930, cannabis extracts were commonly used in various medicinal products. Cannabis was utilized for its potential therapeutic effects, and it was an ingredient in many over-the-counter medications and treatments during that time period. It’s important to note that the regulation and understanding of medicine during this era were quite different from modern standards, and the use of cannabis in medicine was not as tightly controlled as it is today.
Exact numbers can be difficult to determine due to the lack of comprehensive historical records, varying formulations, and changing regulations over time. Cannabis extracts were commonly found in treatments for pain, insomnia, digestive issues, and other ailments. They were often included in tonics, tinctures, and elixirs.
One notable example is the widespread use of cannabis in various forms in the United States Pharmacopeia (USP), a publication that provided standards for the preparation and labeling of medicines. The 1851 and 1916 editions of the USP included cannabis as an ingredient in numerous preparations.
By the early 20th century, concerns about the potential dangers of cannabis, combined with evolving medical understanding, led to its gradual removal from official pharmacopeias and a decline in its use in mainstream medical practice.

Along comes Harry Anslinger. Harry Anslinger was not directly in charge of a single report that deemed cannabis as non-medicinal. However, he played a significant role in shaping the public perception and legal status of cannabis through his role as the Commissioner of the Federal Bureau of Narcotics (FBN), which later became the Drug Enforcement Administration (DEA) in the United States.
During Anslinger’s tenure from 1930 to 1962, he strongly advocated against the use of cannabis and worked to promote the idea that it was a dangerous drug with no medicinal value. He used his influence to push for legislation such as the Marihuana Tax Act of 1937, which effectively criminalized the possession and distribution of cannabis.
There were several factors that contributed to Anslinger’s stance on cannabis:
- Racism and Xenophobia: Anslinger fueled anti-cannabis sentiment by associating it with racial and ethnic minorities, particularly Mexican immigrants and African Americans. He used racially charged language to depict cannabis use as a threat to white society.
- Political and Economic Motivations: Anslinger’s efforts to criminalize cannabis were also influenced by political and economic factors. The FBN needed a cause to justify its existence, and anti-drug campaigns were a way to secure funding and expand its authority.
- Moral and Social Concerns: Anslinger and other proponents of cannabis prohibition believed that its use led to moral degradation and criminal behavior. They argued that it was a gateway drug that could lead to the use of more harmful substances.
- Lack of Scientific Understanding: At the time, there was limited scientific research on cannabis and its potential medical benefits. Anslinger capitalized on this lack of understanding to push his anti-cannabis agenda.

What Prevents The U.S. Government From Taking A Stance On Cannabis As A Medicinal Plant
While some progress has been made in acknowledging the potential medical benefits of cannabis, there are still several factors that have contributed to historical resistance or reluctance to fully embrace its medical use:
- Historical Perspective: Cannabis was classified as a schedule I controlled substance under the Controlled Substance Act of 1970, which categorized it as having a high potential for abuse and no accepted medical use. This classification has made it difficult for researchers to conduct comprehensive clinical trials to establish its medical benefits.
- Lack Of Scientific Research: Due to its Schedule I status, researchers have faced numerous legal and bureaucratic barriers to conducting rigorous scientific studies on the medical benefits of cannabis. Limited research availability has made it challenging to gather enough evidence to support its medicinal use.
- Social and Cultural Factors: Cannabis has long been associated with recreational use and has carried a stigma due to its psychoactive properties. This stigma has influenced public opinion and policy decisions surrounding its medicinal use.
- Pharmaceutical Industry and Competition: The pharmaceutical industry, which plays a significant role in shaping healthcare policy, may view cannabis as a potential competitor to their products. This could influence lobbying efforts and policy decisions.
- Political Considerations: Cannabis legalization, even for medicinal purposes, can be a contentious political issue. Policymakers may be concerned about potential backlash or misperceptions among their constituents.
- International Treaties: The U.S. is a signatory to international drug control treaties that classify cannabis as a controlled substance. These treaties could limit the government’s ability to fully acknowledge its medicinal benefits without potentially violating international agreements.
- State-Level Variability: While some states have legalized medical cannabis and recognized its benefits, there is still no consistent federal approach. This patchwork of state-level laws creates a complex regulatory landscape.
Its worth noting that there has been some positive movement on this issue in recent years. For example, the 2018 Farm Bill legalized the cultivation of hemp, a non-psychoactive variety of cannabis, which opened the door to increased research and the production of CBD-based products. Additionally, the U.S. Food and Drug Administration (FDA) has approved some cannabis-derived medications for specific medical conditions, such as Epidiolex for certain forms of epilepsy.
Public opinion has also shifted in favor of medical cannabis, and as more research becomes available, there might be greater acknowledgment of its potential benefits by the U.S. government. We will stay tuned in and alert our readers with the most up-to-date information on this topic, as opinions and policies evolve.